
Hyponatremia Consults
Hyponatremia is a common electrolyte derangement that you will see on the nephrology consult service. It can be associated with high rates of morbidity and mortality, especially in severe cases. When consulting for hyponatremia, it is essential to evaluate the most likely etiology in order to appropriately manage these patients.
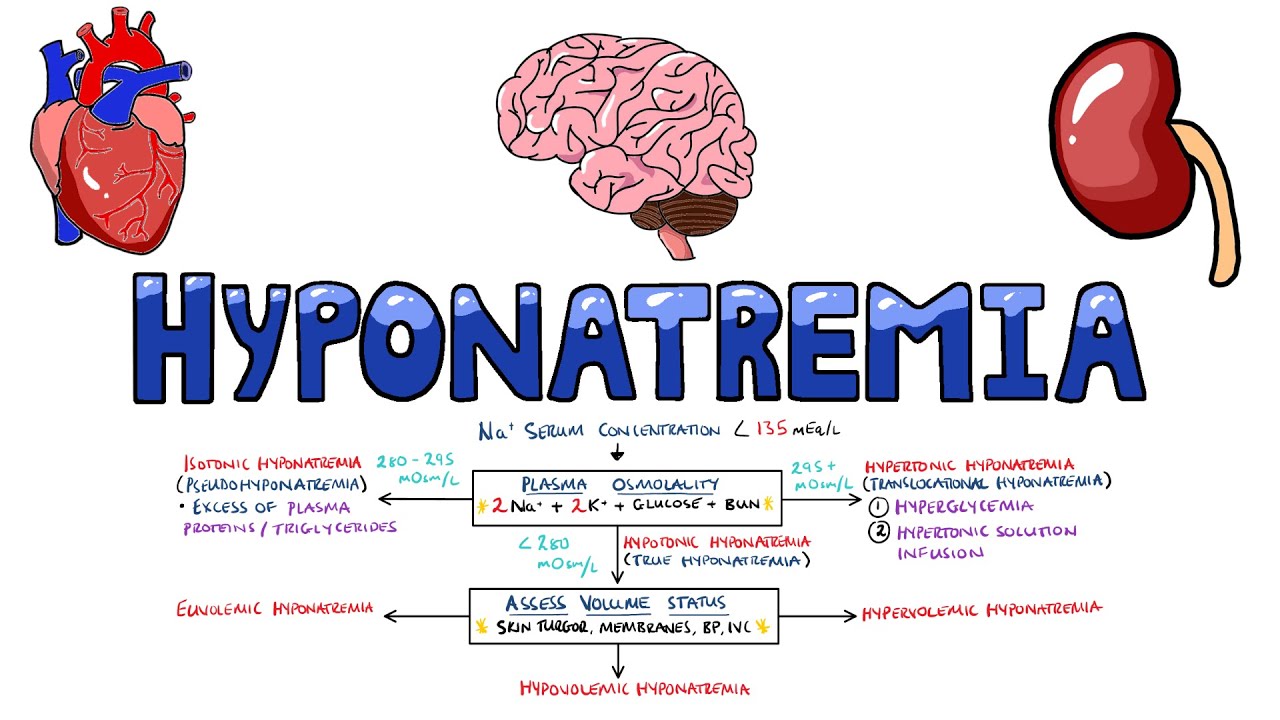
Physiologic Approach to Hyponatremia
by John Roberts
This video lecture is an overview of how to think through hyponatremia physiology
Skeleton Key Group Case #24: Why So Sad, Sodium?
by Sai Achi
The Skeleton Key Group, a team of 50-odd nephrology fellows who work together to build a monthly education package for the Renal Fellow Network. The cases are actual cases (without patient identifying information) that intrigued the treating fellow.
The following exercise will take you through a classic hyponatremia case, as well as highlight the algorithm for deducing the etiology.
Severe hyponatremia
Written by: Jim O’Brien, MD
Edited by: David Kaltman, MD
Expert Commentary by: Sarah Dhake, MD & Josh Waitzman, MD, PhD
Many patients you will be consulted for will already have received treatment for hyponatremia prior to the consult, often in the emergency department and/or ICU setting. This post takes you through the emergency management of hyponatremia and the role for nephrology in these cases.
Hypertonic Saline and Desmopressin: A Simple Strategy for Safe Correction of Severe Hyponatremia
by Lonika Sood MD, Richard H. Sterns MD, John K. Hix MD, Stephen M. Silver MD, Linlin Chen PhD
Desmopressin (“the DDAVP clamp”) has become more commonly used to prevent rapid overcorrection of hyponatremia in the ICU setting. This paper helped establish the role of DDAVP-this is more in-depth than needed, but it will give you background for the use of DDAVP.
REBOOT #48 Hyponatremia Deconstructed
with Joel Topf, MD
Finally, if you’d like to hear a discussion of hyponatremia from etiology to management, consider listening to this podcast.